
Examining the nasal turbinates as a potential source of obstruction in a pediatric Down syndrome patient.
 |
When a pediatric patient with Down syndrome presents with obstructive sleep apnea (OSA), multiple sources of obstruction are routinely examined, but the nasal turbinates are not a traditional area of focus. Though not a typical focal point, the nasal turbinates are a potential source of obstruction in this patient population and therefore require attention. The case of an obese 7-year-old Down syndrome patient with OSA is a testament to the value of thorough examination of the nasal turbinates. After noting the source of obstruction, the patient underwent Coblation turbinate reduction and adenoidectomy, resulting in significant improvement in sleep, respiration, and gas exchange.
BACKGROUND
There is a high prevalence of OSA in children with Down syndrome, of which there are many potential causes, including muscular hypotonia, congenital subglottic stenosis, lymphoid hyperplasia, laryngomalacia, tracheal stenosis, midfacial hypoplasia, and micrognathia.1-3 Additionally, a characteristic trait experienced by children with Down syndrome is tongue enlargement accentuated by their general hypotonia, which can lead to airway obstruction.4 Polysomnography studies have shown that pediatric Down syndrome patients have a significantly reduced arousal index, elevated median apnea-hypopnea index (AHI), and elevated median desaturation index (DI). Untreated OSA may further impair mental function in children with Down syndrome, so timely diagnosis and management are critical. As children with Down syndrome have difficulty complying with continuous positive airway nasal pressure (CPAP) therapy, surgical treatment aimed at correcting both the anatomic soft-tissue and skeletal deformities associated with upper airway obstruction may be necessary in order to improve sleep and respiratory problems.5
 |
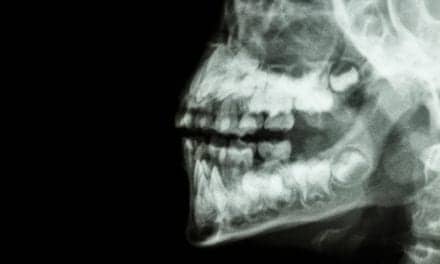
| Figure 1. X-ray of lateral neck showing adenoid enlargement/regrowth with partial obstruction of the nasopharyngeal airway. |
Traditional techniques utilized for surgical management of hypertrophied turbinates include cold-steel turbinectomy and turbinoplasty, cryosurgery, laser, electrocautery, microdebridement, and outfracture of the inferior turbinate. However, these techniques have been linked to complications such as high postoperative bleeding rates and a chronic dry, crusty nose due to altering of the nasal mucosa. Although generally accepted for treating adults, these procedures have the potential to change intranasal architecture and destroy healthy tissue, which can negatively impact facial growth. In my experience, turbinate reduction utilizing Coblation technology is a less invasive procedure that has provided positive results while enabling the preservation of the critically important nasal mucosa.
PHYSICAL EXAMINATION
The patient, a 7-year-old white male with autism, Down syndrome, celiac disease, obesity (38.8 kg, 110 cm, BMI = 32), and a history of atrial septal defect, was evaluated for OSA in June 2009 because his symptoms continued to increase despite undergoing a tonsillectomy and adenoidectomy in May 2006. X-ray examination revealed adenoid regrowth, and physical examination showed hypertrophied nasal turbinates contributing to obstruction (Figure 1). The patient was noncompliant with CPAP therapy and experienced an O2 saturation of 50%.
POLYSOMNOGRAPHY
 |
| Table 1. Respiratory and gas exchange analysis pre- and post-Coblation procedure. |
A sleep laboratory study performed in June 2009 during the patient’s habitual sleep period revealed OSA with an AHI of 24. His total sleep time was 450 minutes, with 19% total rapid eye movement (REM) comprised of stage N1, N2, and N3 sleep of 3%, 36%, and 42%, respectively. There was significant sleep fragmentation; the patient awakened 14 times and had 54 arousals (arousal index = 7). There were delays in his sleep onset, stage 2 sleep, and REM sleep of 17, 17, and 86 minutes, respectively. Snoring was noted throughout the night.
Respiratory analysis revealed 65 obstructive and 0 mixed apneas. There were 118 hypopnea episodes observed during the course of this study. The REM apnea-hypopnea index was 66. The mean oxygen saturation during NREM was 90% and during REM sleep was 84%; 42% (190 minutes) of the entire study time was spent with an oxygen saturation of <90%.
MANAGEMENT
In July 2009, a revision adenoidectomy and turbinate reduction was performed utilizing Coblation to address the patient’s OSA. Total procedure time required about 20 minutes and resulted in very little blood loss and minimal damage to surrounding normal tissue. The patient was admitted to the hospital postoperatively for overnight monitoring, but required no supplemental oxygen, and was discharged home the following day. His parents noted return to normal activity and diet within 48 hours of surgery.
FOLLOW-UP AND OUTCOME
In October 2009, the child underwent a polysomnography that demonstrated a decline in arousals to 33, resulting in a reduced arousal index from 7 to 5. Respiratory analysis showed a dramatic reduction in the number of obstructive apneas from 65 to 8, and the number of observed hypopnea episodes significantly decreased from 118 to 59 during the course of this study. The apnea-hypopnea index decreased from 24 to 9, and the REM apnea-hypopnea index decreased from 66 to 20.
The child’s total sleep time was 436 minutes, with a sleep and stage 2 latency of 8 minutes each, and latency of REM of 69 minutes. Stage N2 sleep increased to 58% and stage N3 sleep decreased to 26%.
Postprocedure gas exchange showed that the lowest O2 saturation was now 78%. The mean oxygen saturation during NREM remained constant at 90%, and the oxygen saturation increased during REM sleep from 84% to 91% (Table 1).
DISCUSSION
Following Coblation surgery in July 2009, the patient experienced significant clinical improvements in sleep, gas exchange, and respiration despite the fact that he continues to experience minor sleep apnea. The patient was discharged with instructions to sleep on his side and was placed on 0.5 liters of supplemental oxygen by nasal cannula in the evenings. He was also advised to take melatonin to help regulate sleep and wake cycles.
The positive results achieved in this case emphasize the importance of routinely examining the nasal turbinates as a potential source of obstruction in this patient population. Coblation technology provides a more rapid procedure, with an easier recovery and reduced side effects as a result of the minimal damage to surrounding tissue and reduced intraoperative blood loss.6 The lower-temperature technique allows for the reduction of the turbinates without altering the nasal mucosa, enabling the preservation of normal nasal function and facial growth. Another notable advantage of Coblation turbinate reduction is the brevity of the procedure. The aggregate series of passes of the Coblation probe into the turbinate take a total of 60 seconds to complete per side.7,8
Meredith N. Merz, MD, is a member of the Department of Otolaryngology at Nationwide Children’s Hospital in Columbus, Ohio. She has clinical interests in general pediatric otolaryngology, head and neck and thyroid masses, obstructive sleep apnea and other airway problems, and disorders of the ears and nose. Her research interests include treatment of recurrent respiratory papillomatosis, obstructive sleep apnea, and nasal airway obstruction. The author can be reached at [email protected].
Letter to the Editor in Response to “Sniffing Out the Obstruction”
Dear Editor,
I am writing in response to the article “Sniffing Out the Obstruction” by Meredith Merz, MD, in the March 2010 issue of Sleep Review magazine. First of all, I applaud Dr. Merz for bringing attention to pediatric sleep disorders and for increasing awareness that surgical procedures, such as Coblation turbinate reduction, can significantly reduce the severity of sleep-related breathing disorders in children. However, I was disappointed to read that Dr. Merz felt that post-operatively the child in this case had only “minor sleep apnea,” despite a post-operative AHI of 9.0. Although this was a significant improvement, an AHI of 9.0 is still very significant in a child. Even for an adult, such an AHI is associated with a diagnosis of obstructive sleep apnea (OSA). Therefore, I was disheartened to see that Dr. Merz missed an opportunity to completely treat this child for OSA to fruition. Unfortunately, Dr. Merz discharged the patient with supplemental oxygen therapy and melatonin, neither of which is a recognized treatment for OSA. After getting such a good result with Coblation turbinate reduction, this child would probably have benefited from another trial of CPAP therapy. Because of the significant improvement in nasal airway patency, the child in this case would probably be much better able to tolerate CPAP treatment.. This approach would ensure adequate and successful long-term treatment of OSA. This brings up another important point, that OSA is a chronic medical condition and it should be managed as such. The longer those of us in the physician community fail to understand that, the longer we will see epidemic rates of childhood obesity in this population. I hope that Dr. Merz will follow-up with this patient and consider a re-trial of CPAP therapy to fully and optimally treat this child’s significant and persistent OSA. I also hope that other physicians treating children will become more aware of the importance of fully treating OSA as a chronic medical condition and the greater need for regular follow-up care.
Sincerely,
Raj Kakar, MD, MPH, FAASM
Board-Certified, Internal Medicine and Sleep Medicine
President & C.E.O., The Dallas Center for Sleep Disorders
6313 Preston Road, Suite 400
Plano, TX 75024
The author replies:
Dear Dr Kakar,
Thank you for the comments regarding the recent case study reported in Sleep Review. I appreciate the points you raise, and I agree that it is incorrect to label this patient’s postoperative result as “minor sleep apnea”. Because of length limitations, details of this patient’s postoperative sleep study were not included in the case study. The overall AHI postoperatively was 9; however the sleep study was actually performed as a split-night study, where he was placed on 0.5 L nasal cannula part-way through the night. After being placed on the supplemental oxygen, the AHI dropped to around 1 and the patient’s lowest oxygen saturation was 90%, therefore it was felt that the combination of the surgical intervention with this subsequent intervention did adequately treat the sleep apnea in this patient. CPAP was not attempted again because, in this patient with Down Syndrome and autism, intolerance was thought related to his behavioral issues and not simply his nasal obstruction. Of note, the patient is also obese and suffers from Celiac disease. His family continues to work on weight loss. I worked extensively with our sleep medicine physician here regarding this patient’s postoperative care, and we certainly do agree that OSA in this patient population is a chronic condition. We do not feel that this patient is “cured”. As he becomes older, we will continue to reassess and to reevaluate whether CPAP is a viable option for him.
I thank you again for your comments. Please feel free to contact me with any other questions or comments.
Meredith Merz, MD
REFERENCES
- Marcus CL, Keens TG, Bautista DB, von Pechmann WS, Ward SL. Obstructive sleep apnea in children with Down syndrome. Pediatrics. 1991;88:132-9.
- Ng DK, Hui HN, Chan CH, et al. Obstructive sleep apnea in children with Down syndrome. Singapore Med J. 2006;47:774-9.
- Jacobs IN, Gray RF, Todd NW. Upper airway obstruction in children with Down syndrome. Arch Otolaryngol Head Neck Surg. 1996;122:945–50.
- Guimaraes CV, Donnelly LF, Shott SR, Amin RS, Kalra M. Relative rather than absolute macroglossia in patients with Down syndrome: implications for treatment of obstructive sleep apnea. Pediatr Radiol. 2008;38:1062-7.
- Erler T, Paditz E. Obstructive sleep apnea syndrome in children: a state-of-the-art review. Treat Respir Med. 2004;3(2):107-22.
- Glade RS, Pearson SE, Zalzal GH, Choi SS. Coblation adenotonsillectomy: an improvement over electrocautery technique? Otolaryngol Head Neck Surg. 2006;134:852-5.
- Back LJ, Hytonen ML, Malmberg HO, Ylikoski JS. Submucosal bipolar radiofrequency thermal ablation of inferior turbinates: a long-term follow-up with subjective and objective assessment. Laryngoscope. 2002;112:1806-12.
- Bhattacharyya N, Kepnes LJ. Clinical effectiveness of coblation inferior turbinate reduction. Otolaryngol Head Neck Surg. 2003;129:365-71.



{kind=link}