
By implementing an automatic referral system in its EMR software, Parrish Healthcare Center creates a win-win for its sleep center and affiliated hospital, all while better managing patient health.
Today healthcare is no longer a fee-for-service operation. Providers are being graded on how they can improve patients’ quality of life, reduce exacerbations, reduce emergency department visits and/or hospitalizations, reduce expenditures for medical care, and allow patients to lead more active and productive lifestyles.
In this new way of thinking, sleep centers need to adapt to survive. We need to start thinking of ourselves as part of an integrated part of our patient’s healthcare.
Formerly, as a paramedic, I noticed most of our heart attack calls were between 4 AM and 5 AM. I never understood why until I started working in a sleep center and realized that this corresponds to the time of a patient’s last and longest REM cycle, when sleep apnea becomes significantly worse. The patient’s oxygen saturations fall and make him or her more susceptible to arrhythmias, myocardial infarctions, and premature cardiac death.
Our hospital is presenting many process-improvement plans to reduce readmissions, shorten length of stay, and set goals to better manage our patient care. The sleep center can help. The sleep center can help save the hospital money and at the same time increase referrals.
With home sleep testing on the rise, I needed to come up with ways to both grow the sleep center’s patient volume and help prevent readmissions at the hospital. With these goals, I came up with an automatic referral system that we implemented into our electronic medical records (EMR) software. This system is an automated process where we screen hospital-based patients on their comorbid conditions.
I recognized that the process for screening patients needed to be automated and effortless. I needed to devise a way to be alerted of the high-risk patients being admitted but without causing extra work to the nursing staff.
I worked with our health information management team to create a consult alert for patients with specific comorbid conditions (based on their active diagnosis, as well as their past medical history). We implemented this alert into our Meditech 6.0 EMR so seamlessly that the nurses aren’t even aware that it’s being done.
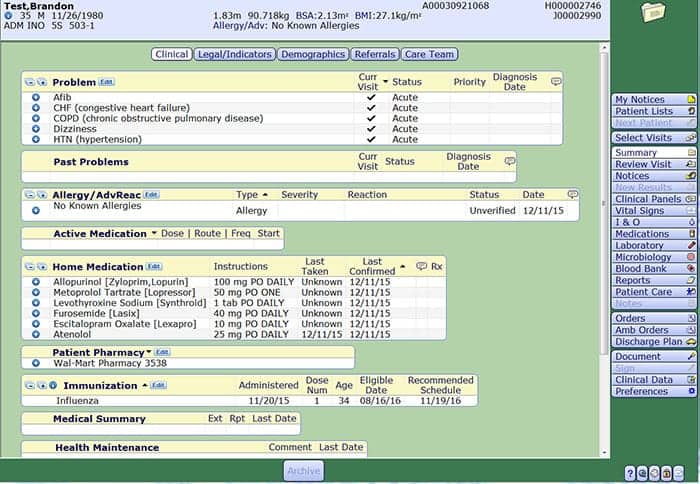
This EMR summary page (filled here with fictitious information) shows the current visit problems, which can trigger a notification for a sleep consult.
The way it works is that when a patient arrives on a floor, the nurse completes an admission assessment, which contains questions regarding past medical history. The built-in intervention in the EMR triggers an alert when patients have certain comorbid conditions. The conditions we have the EMR flag are those for which there are evidence-based studies that show exacerbations linked to untreated sleep apnea. (More and more studies are being done linking untreated sleep apnea to an increase in mortality, length of stay, and readmissions.) Any patient with a diagnosis of heart failure, stroke, BMI greater than 40, COPD, and arrhythmias will trigger a sleep consult recommendation. This consult alerts the sleep center of a patient’s need to be screened for sleep apnea and is automatically printed to the sleep center from the EMR.
Originally, the sleep center called these high-risk patients after they were discharged. However, a majority of patients thought the sleep center was trying to sell them a service. Common discharged patient responses included “No one talked to me in the hospital about this!” and “Why are you calling me now?” Unsurprisingly, we had a very high refusal rate.
Those refusals made me realize that these patients needed to be contacted while they were still in the hospital, and we would need a rounding sleep technician to do that. Dubbed our Sleep Navigator, this person would use the screening tools that we built in our EMR—which are comprised of a list of the patient’s comorbid conditions, the Epworth Sleepiness Scale, Berlin Questionnaire, STOP-Bang Questionnaire, questions about sleep hygiene, and questions regarding symptoms like shortness of breath while supine and frequent nighttime urination. After the screening, the Navigator would mark the patient as low or high risk.
We did not want to do a STOP-Bang or simple Berlin on all admissions because we would be getting too many false positives since the questionnaire is so subjective. Plus the STOP-Bang and Berlin measure the risk mainly for obstructive sleep apnea, and we needed a screener that can screen the risk for central apneas as well—especially since heart failure is the leading comorbid condition for readmissions and heart failure patients are more at risk for central apneas.
I knew that my hospital administration would need evidence to prove the value of another full-time employee. So for 2 months, working more than 12 hours a day, I screened patients while also managing a high-volume sleep center. I did that to prove that this position would pay for itself. In those 2 months, we saw an extra 26 patients, and 19 of those were positive for moderate to severe sleep apnea. Seeing these results, administration approved the position. The Sleep Navigator now rounds on patients Monday to Friday from 8 AM to 4 PM.

Kristina Weaver, RPSGT
In the first year of the program, from October 2014 to October 2015, a total of 176 studies were completed, resulting in a third of our total volume of studies being referred from our Sleep Navigator with 86% positive for sleep apnea.
Once the Navigator determines the patient is at high risk, she makes a note in the sleep screening section in the EMR and refers the patient for an outpatient sleep consultation with the sleep specialist. The consultation can occur in the sleep center or directly in the physician’s office as an outpatient appointment. We found there was much more success if the patient was scheduled prior to being discharged. The appointment should be a part of the patient’s discharge packet.
The sleep specialist then does a face-to-face consultation and, if he or she agrees that the patient would benefit from a sleep study, writes the order for the exam. The patient is referred to a sleep center that is in-network with his or her insurance.
We are a small not-for-profit hospital with approximately 200 beds. I have personally educated the hospitalists, cardiologists, those in the heart failure group, and many more. After this education, the specialists are now more acutely aware of the complications sleep apnea can cause. We have seen admissions directly linked to sleep apnea.
This process helps increase revenue and volume to the sleep center and routinely makes up for the studies that insurance companies deny due to stricter authorizations and a move to home sleep testing.
Our goal is to help the patients manage their comorbid conditions by better managing their sleep apnea, which will result downstream in a lesser risk for readmission.
Kristina Weaver, RPSGT, is neurodiagnostic manager at Parrish Healthcare Center in Port St John, Fla. She is also president of the Florida Association of Sleep Technologists and Brevard A.W.A.K.E. coordinator. The article is her own and does not necessarily reflect the views of Parrish Medical Center.



{kind=link}
Great job Kristina!!! Another example of how you think outside the box to improve the health of sleep apnea patients whether already diagnosed or for those who are undiagnosed. Your passion is inspiring!
Thank you!!!!
Great article, Kris.
Thank you!!!!
Kristina, This is quite innovative and forward -thinking. thank you and congratulations on your great work. I plan to share with my local sleep centers. May I?
Jim Doc Hales 4-3-16 dental sleep medicine